last updated:
March 13, 2026
min read
What causes PCOS?




Knowing what causes PCOS matters more than you think: It explains why symptoms show up the way they do and why personalized treatment—not guesswork—makes all the difference.
People often ask “what causes PCOS?” expecting a single root problem. What they usually find instead is there’s no clear-cut answer, which can feel discouraging—but don’t give up.
I’ve been there myself: While I don’t have polycystic ovary syndrome (PCOS), I do live with chronic health issues that aren’t tidy or easily explained—conditions driven by multiple overlapping factors with no single smoking gun. That kind of uncertainty can make you feel isolated, frustrated, and desperate for a simple cause-and-effect story. So when people hear, “We don’t know what causes PCOS,” it can feel like a dead end.
But the reality is more nuanced than that: no single cause doesn’t mean no understanding; it means PCOS is complex. Thus far, research points to PCOS as a condition shaped by several interconnected systems working together. While there’s still a lot we don’t know, our understanding of PCOS causes–including PCOS hormone levels, metabolism dysfunction, and other risk factors–has evolved dramatically in recent years.
In this article, we’ll break down what science actually shows about PCOS—whether PCOS is genetic, how hormones and metabolism interact (along with environmental factors) and why symptoms can look wildly different from one person to the next. Most importantly, we’ll connect the dots between what causes PCOS and what that means for real-world care, symptom management, and long-term health.
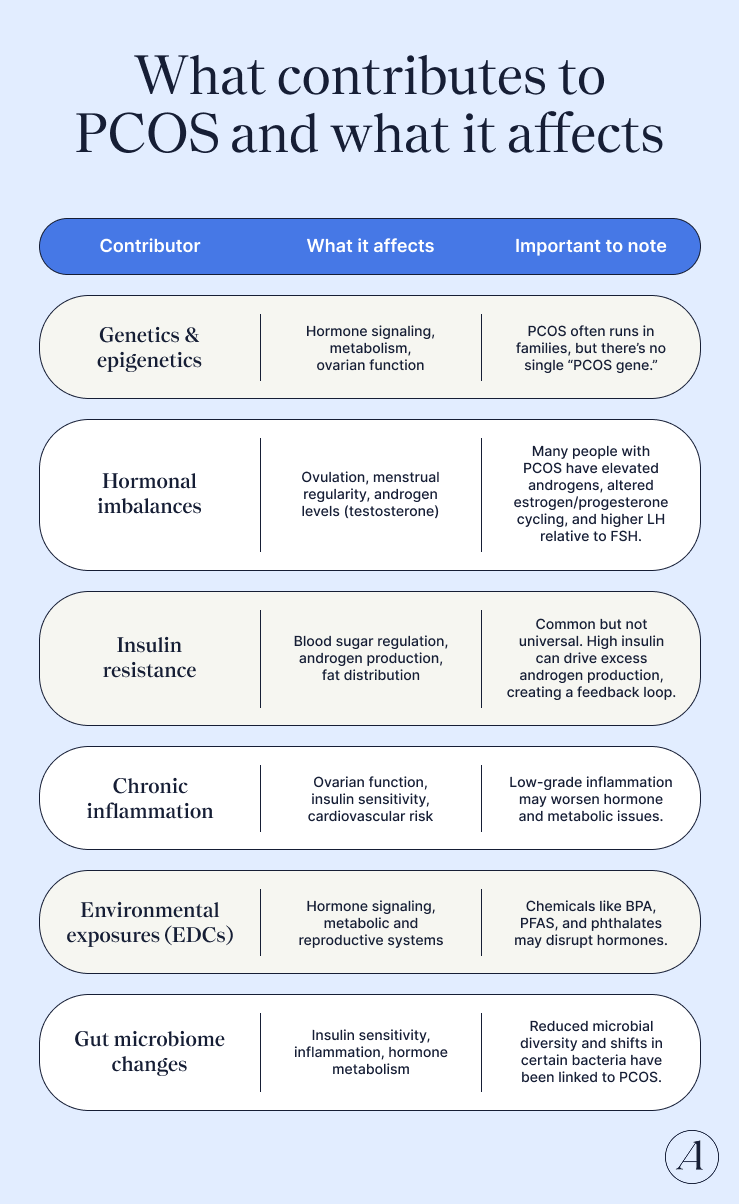
PCOS doesn’t have one single cause. It’s what experts call a multifactorial condition, meaning several biological systems overlap and interact. “PCOS is a multifactorial disorder that stems from genetic variances, environmental exposures, metabolic factors, and epigenetic modifications,” says Gouri Pimputkar, DO, FACOG, DipABLM, clinical lead at Allara Health. In other words, there isn’t one starting point—there’s a network of influences that build on each other over time.
The most likely contributors include:
Think of PCOS less as one problem and more as a perfect storm of factors, and the mix looks a little different for everyone. Up next, we’ll break down what the science says about each of these contributors and how they may fit together.
Is PCOS hereditary? If your mom, aunt, or sister has PCOS—or even type 2 diabetes—your own risk may be higher. While the exact cause of PCOS is still unknown, research consistently shows that genetics play a meaningful role. In fact, twin studies estimate that about 72% of PCOS risk may be genetic.
Other data shows that “daughters of women with PCOS have more follicles on their ovaries and metabolic abnormalities that present from infancy through adolescence, well before actual clinical symptoms appear,” says Dr. Pimputkar.
That said, PCOS isn’t caused by one “bad gene.” It’s a polygenic, multifactorial condition, meaning risk is shaped by many genes working together, along with environmental factors. Scientists know genetics matter, but there’s still no single genetic test or marker that can definitively predict PCOS.
There’s still so much we don’t understand about what’s behind PCOS, but here’s what the research says so far:
Researchers have identified gene variants linked to PCOS
Through large genome-wide association studies, 21 genetic risk loci for PCOS (in people of European and Han Chinese backgrounds) have been discovered. These include genes related to:
Genetics may explain why PCOS doesn’t look the same in everyone
This wide genetic spread helps explain why PCOS affects both hormones and metabolism, plus why symptoms can look so different from person to person.
Using genome-wide association studies, researchers have identified four genetic “clusters” of PCOS, each tied to a different symptom pattern:
In other words: your genetic makeup may shape how PCOS shows up for you.
Epigenetics may affect who develops PCOS too
Beyond inherited genes, epigenetic changes—which affect how genes are turned on or off—also seem to matter. “Some studies show that the environment can influence PCOS through epigenetic modifications that can be transmitted through generations,” says Dr. Pimputkar. For example, animal studies suggest that higher androgen exposure during fetal development may increase the risk of PCOS-like symptoms later in life, potentially across generations. Factors like maternal obesity or smoking may also shape the uterine environment in ways that raise long-term PCOS risk, she adds.
Many people with PCOS have problems with insulin, the hormone that helps move glucose from the bloodstream into cells for energy. Some estimates suggest 35%-80% of those with PCOS also have insulin resistance. When the body becomes insulin resistant, cells stop responding efficiently, forcing the pancreas to pump out more insulin to keep blood sugar in check.
That insulin overload can set off a hormonal chain reaction, directly disrupting reproductive hormones. For example, “higher levels of insulin indirectly increase the amount of circulating androgens as well as directly stimulate the adrenals and ovaries to make more,” says Dr. Pimputkar. Everyone produces androgens like testosterone (even though they’re often called “male hormones”), but when levels run too high, they can throw things off balance. This hyperandrogenism is behind many hallmark PCOS symptoms, including acne, excess facial or body hair (hirsutism), and hair thinning on the scalp.
Too much insulin also disrupts signaling in the brain. “There is also an increase in the pulse frequency of gonadotropin-releasing hormone (GnRH), which leads to an over-secretion of luteinizing hormone (LH) relative to follicle-stimulating hormone (FSH),” says Dr. Pimputkar. That skewed LH-to-FSH ratio further fuels androgen production, she adds.
The ripple effects don’t stop there. When LH outweighs FSH, follicles struggle to mature properly, says Dr. Pimputkar. This results in multiple follicles building up in the ovaries, increasing ovarian size and raising anti-Müllerian hormone (AMH) levels. Unfortunately, that rise in AMH helps sustain the high-androgen state, creating a frustrating, self-perpetuating cycle, she explains.
Insulin also lowers levels of sex hormone–binding globulin (SHBG), the protein that normally keeps androgens in check. With less SHBG, more “free” and biologically active androgens circulate in the body, further worsening symptoms. Those elevated androgens can, in turn, promote more insulin resistance, creating another frustrating feedback loop.
Some studies also link these higher androgen levels to increased abdominal and visceral fat in PCOS.
Important to note: While insulin resistance, obesity, and PCOS are connected, not all people with PCOS and insulin resistance will have extra body weight. In fact, PCOS shows up in different phenotypes, including both overweight and lean presentations. People with lean PCOS may not have excess weight, yet still show hormonal, metabolic, and blood-marker differences compared to those without PCOS.
The takeaway? Insulin resistance is common in PCOS, but it doesn’t always look the same and it’s not universal. Think of it as a key contributor for many, not a single root cause for all.
Elevated insulin—and insulin resistance—sit at the heart of PCOS hormone chaos, but they’re not acting solo. “PCOS is not caused by a single hormonal imbalance, but rather multiple interrelated hormonal abnormalities,” says Dr. Pimputkar.
Common hormonal issues seen in PCOS include:
So where does all of this start? Researchers believe many of these hormone shifts stem from dysregulation of the hypothalamic–pituitary–ovarian (HPO) axis—the hormone feedback loop that coordinates ovulation and sex hormone production.
Here’s how that system works when things are running smoothly: The hypothalamus releases gonadotropin-releasing hormone (GnRH), which signals the pituitary gland to produce luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Those hormones then tell the ovaries when—and how much—to produce estrogen, progesterone, and testosterone.
In PCOS, that rhythm can get thrown off at multiple points, including the brain, the pituitary, the ovaries themselves, or all three. A dysregulated HPO axis may look like this:
Understanding this system-wide imbalance helps explain why PCOS isn’t “just an ovary issue,” and why treatment often needs to address more than one hormone at a time.
Chronic systemic inflammation is known to contribute to metabolic diseases like diabetes, which are also more common in people with PCOS. Increasingly, low-grade, chronic inflammation is seen as a key player in the genesis of PCOS as well.
Research backs this up. Studies show that people with PCOS often have moderately elevated levels of C-reactive protein (CRP), a marker of inflammation (even when obesity isn’t a factor). Other research has found increased immune cell activity (including macrophages and lymphocytes) and higher levels of inflammatory messengers like IL-6 and TNF-α. These changes don’t just affect the reproductive system in PCOS; they show up in the cardiovascular system, liver, gut, thyroid, and even the brain.
So where is the inflammation coming from? The answer isn’t simple, but a few theories stand out.
To complicate things further, PCOS inflammation may be a two-way problem. It’s not just an increase in inflammatory signals; there may also be fewer protective ones. Some studies in people with PCOS show lower levels of adiponectin, an anti-inflammatory hormone that also supports metabolic health. Others have found reduced Pentraxin-3 (PTX3), a molecule involved in regulating inflammation and protecting against cardiovascular disease.
Growing evidence suggests that environmental pollutants, especially endocrine-disrupting chemicals (EDCs), may “alter reproductive hormones” in ways that raise the risk of PCOS, says Dr. Pimputkar. These chemicals can mimic or block natural hormones, throwing finely tuned systems off balance.
Here’s what the research is starting to show:
Not everyone exposed to EDCs develops PCOS, but some people may be more vulnerable to their negative effects. In people with a genetic predisposition for PCOS, early-life or long-term exposure could permanently alter metabolic, reproductive, or neuroendocrine regulation in ways that possibly increase PCOS risk or worsen symptoms over time.
The effects may even echo across generations. Some EDCs are linked to epigenetic changes. These shifts may affect the female reproductive system and could potentially be passed down, raising questions about how environmental exposures today might influence PCOS risk tomorrow.
Emerging research suggests the “gut microbiome plays a major role” in the development of PCOS, says Dr. Pimputkar. When researchers compare people with PCOS to those without it, they consistently find meaningful differences in the makeup of their gut bacteria.
Here’s what the science is starting to show:
So, what’s the connection between gut microbes and PCOS? “The gut microbiome helps regulate many body functions like hormone production and insulin sensitivity,” says Dr. Pimputkar. When gut bacteria are out of balance, it can cause chronic inflammation that affects the intestinal barrier, she explains.
One hypothesis—the dysbiosis of gut microbiota (DOGMA) theory—attempts to tie this together. The DOGMA theory suggests that an imbalanced gut microbiome may increase gut permeability. This allows bacterial toxins like lipopolysaccharides (LPS) to enter the bloodstream, activating the immune system. That immune response may interfere with insulin signaling, drive higher insulin levels, increase ovarian androgen production, and disrupt how normal follicles in the ovaries form.
One key example illustrates this theory: bile acids. In people with PCOS, shifts in gut bacteria can disrupt bile acids, which may lower immune molecules that help support healthy ovarian function and insulin sensitivity, says Dr. Pimputkar.
While these findings point to a compelling link between gut health and PCOS, we still need more data to figure out whether targeting the gut microbiome could one day become part of PCOS treatment.
Despite the stereotypes, PCOS doesn’t come in one predictable package. Some people deal with irregular periods and elevated testosterone. Others struggle with insulin resistance and darkened patches of skin. Some have weight gain; others are lean. Same diagnosis—very different day-to-day realities.
That’s because PCOS is a “heterogeneous” condition (science-speak for highly variable symptoms). And contrary to outdated assumptions, PCOS can affect people of all body sizes, shapes, and weights.
So why the wide range? Because PCOS is shaped by multiple forces working together.
How it shows up in your body depends on a mix of factors—genetics, hormone regulation, insulin sensitivity, chronic inflammation, gut microbiota, and even environmental exposures. No two bodies have the same combination. “That is why PCOS comes in all shapes and sizes, with or without insulin resistance and weight gain,” says Dr. Pimputkar.
Genetics offers a clear example of this variability. PCOS doesn’t follow a simple dominant-or-recessive inheritance pattern; instead, it’s influenced by environmental factors that help determine how (or whether) it affects you, says Dr. Pimputkar. “Different combinations of these genetic variations produce different phenotypes of PCOS,” she explains.
In fact, researchers have identified four distinct genetic “clusters” of PCOS, each linked to different symptom patterns and biological pathways. Translation: different bodies may develop PCOS through different dominant mechanisms, which helps explain why symptoms—and treatment responses—can vary so widely.
This is exactly why PCOS care can’t be cookie-cutter. The condition’s complexity calls for individualized treatment that targets the systems driving your symptoms, not someone else’s.
Let’s clear the air—PCOS is not your fault. Despite what the internet (or that one unsolicited relative) might suggest, PCOS isn’t caused by laziness, poor willpower, or eating the “wrong” foods. It’s a medical condition, not a moral failing.
“There are so many interrelated factors contributing to the development and expression of symptoms for PCOS, but blaming the patient for not doing something right or enough is not okay,” says Dr. Pimputkar.
Misinformation doesn’t just confuse; it can actually harm. Conflicting advice about PCOS causes can leave people feeling ashamed or chasing fixes that don’t help (and sometimes make things worse). So let’s be very clear about what doesn’t cause PCOS.
These things do not give you PCOS:
The takeaway: PCOS develops because of complex biological factors, not because you did something wrong. Understanding that distinction is key to moving forward with care that’s grounded in science, not shame.
PCOS is common, so why does it still feel like a medical mystery?
An estimated 11–13% of women worldwide live with PCOS, and its prevalence has roughly doubled over the past 30 years. Yet despite how widespread it is, major gaps remain in how we understand its causes, subtypes, and best treatments.
The uncomfortable truth: PCOS research has been chronically underfunded. Women’s health in general has historically gotten the short end of the research budget. Case in point: In 2020, just 5% of global research and development funding went to women’s health. Of that, 4% focused on women’s cancers, leaving only 1% for all other women-specific conditions, including PCOS.
For decades, women were barely included in science at all. Before 1993, women were routinely left out from clinical trials. It wasn’t until Congress stepped in and made inclusion a legal requirement for NIH-funded research that this began to change. Even today, some researchers avoid using female lab animals because hormonal cycles are considered “too complicated” or expensive to study.
Put it all together, and the slow progress starts to make sense. When a condition is underfunded, understudied, and historically sidelined, breakthroughs take longer. That’s why so much about PCOS—from its root causes to its many subtypes—remains unclear. The good news? Awareness, advocacy, and research momentum are growing. But there’s still a long way to go.
Cracking the “why” behind PCOS could change everything for diagnosis and care.
Right now, even getting a diagnosis can be frustratingly complicated. There’s no single test for PCOS. Instead, providers have to piece together symptoms, lab results, and imaging, while ruling out other conditions that can look similar. That’s because PCOS isn’t one-size-fits-all: it shows up differently in different bodies, which makes diagnosis—and treatment—tricky.
A clearer understanding of what actually drives PCOS would help clinicians identify it earlier and more accurately. Just as important, insights into the disease’s underlying biology could unlock more targeted therapies. Research is already moving in this direction, with studies uncovering new pathophysiologic pathways and treatments now being explored in preclinical and clinical trials.
Because PCOS affects everything from hormones to metabolism to mental health, effective management usually requires a multi-pronged, team-based approach. Many people with PCOS end up seeing several specialists, each addressing a different piece of the puzzle:
The magic happens when those providers actually talk to each other. Interprofessional care—where specialists collaborate and coordinate—is key to better outcomes and safer care. Without it, patients are often left juggling siloed advice and disconnected treatment plans.
That’s where comprehensive care models shine. Programs like Allara’s are built around the complexity of PCOS. They offer integrated testing across endocrine, gynecologic, and metabolic systems, so nothing gets missed. Patients work with a dedicated care team—including board-certified OB-GYNs, endocrinologists, and registered dietitians—who see the full picture. Translation: no fragmented care, no mixed messages, no “figure it out yourself.”
What this means for you: PCOS needs whole-person care. A patient-centered approach that blends medical and nutrition support isn’t just helpful—it’s the most sustainable path to long-term management.
PCOS is a complex, whole-body condition shaped by biology, environment, and lived experience. Understanding what’s behind it helps explain why symptoms show up the way they do and why one-size-fits-all care so often falls short.
The encouraging part? As science gets clearer on PCOS causes, care is getting smarter, more personalized, and more effective. And you don’t have to untangle it alone.
That’s where Allara comes in. The experts at Allara investigate, diagnose, and build a treatment plan that looks at your hormones, metabolism, and symptoms together, so you can stop chasing answers and start feeling back in sync with your body again.
Short answer: no. But it is very treatable, and the right mix of therapies can make a big difference. Treatment is personalized, but these are the most common, evidence-based approaches:
The exact cause of PCOS isn’t fully understood, but experts agree it’s multifactorial—meaning several factors interact rather than one single trigger. Research points to a mix of:
Different combinations of these factors likely explain why PCOS looks so different from person to person.
The most common early red flag of PCOS is irregular or missed periods. That said, PCOS usually isn’t diagnosed until 2–3 years after the first period, since it can take time for cycles to naturally regulate during adolescence.
Other possible early signs include:
If these symptoms sound familiar, it’s worth talking to a healthcare provider. Early recognition can make management much easier.
“I was given an explanation of how my hormonal imbalance was affecting me as a whole - body & mind - & tools so that we could start to manage my condition. I am happy to announce after a year of trying, I found out that I was pregnant & I couldn’t be happier!”


“This is genuinely the first time in my 7 years of being diagnosed, that I have felt seen and heard.”

“The Allara Community gives me the courage and support to continue my PCOS journey - I am never afraid to ask the hard questions and love hearing from other women with the same challenges.”

"My doctor went above and beyond making sure I had all the necessary tests, but also tremendously helped me in understanding my diagnosis, helping me change my lifestyle, and making sure I get the treatment I deserve."

"Before Allara I had no real direction or understanding of what it meant to have PCOS. Now I have a team of people that take time to explain every single thing to me, ask me how I feel and let me be a part of my treatment plan."
